
According to HIPAA Journal, 710 US healthcare breaches affecting at least 61.5 million individuals were reported in 2025 alone. Unsecured communication channels are a contributing factor that practices routinely overlook.
This guide covers what HIPAA actually requires of a VoIP system, which security features are non-negotiable, what a Business Associate Agreement does, and how to evaluate a provider before you sign.
Key Takeaways
- HIPAA-compliant VoIP depends on technical controls, vendor agreements, and internal policies working together.
- A signed Business Associate Agreement (BAA) from your VoIP provider is legally required before using the system for patient communications.
- End-to-end encryption, role-based access controls, and audit trails are non-negotiable in a compliant healthcare VoIP system.
- Evaluate VoIP systems on compliance depth and workflow fit, not price or feature count alone.
What Is Secure VoIP for Healthcare?
VoIP (Voice over Internet Protocol) routes calls over the internet rather than copper telephone lines. "Secure VoIP for healthcare" refers to systems configured with the additional privacy, encryption, and auditability controls required in regulated clinical environments. That's a meaningfully different product than consumer or generic business VoIP.
A healthcare VoIP system typically covers:
- Inbound and outbound patient calls
- Voicemail storage and retrieval
- Call recording and transcription
- Fax and SMS appointment reminders
- Telehealth voice and video
- Multi-site call routing
Every one of these functions can touch PHI. HHS has confirmed that the HIPAA Security Rule applies to PHI transmitted through VoIP, cellular, and Wi-Fi — unlike traditional landline audio, which falls outside the Security Rule's electronic transmission scope.
VoIP is not inherently HIPAA-compliant. Compliance comes from deliberate configuration, vendor agreements, and documented internal policies.
Why Standard VoIP Puts Healthcare Providers at Risk
Standard business VoIP systems — and especially consumer-grade options — lack the encryption standards, audit logging, and access controls required under the HIPAA Security Rule. Calls can be intercepted. Voicemails are often stored without encryption.
Most standard providers won't sign a Business Associate Agreement (BAA), which makes using their system for patient communications a HIPAA violation regardless of any other precautions you take.
The Real Financial Exposure
HHS's 2026 civil monetary penalty structure sets four culpability tiers:
| Culpability Tier | Minimum Per Violation | Maximum Per Violation |
|---|---|---|
| Did not know (and reasonably couldn't have) | $145 | $73,011 |
| Reasonable cause, not willful neglect | $1,461 | $73,011 |
| Willful neglect, corrected in time | $14,602 | $73,011 |
| Willful neglect, not corrected | $73,011 | $2,190,294 |
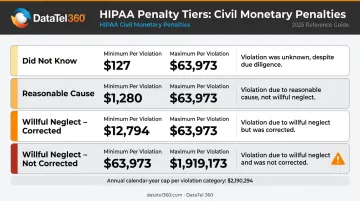
The calendar-year cap for identical violations is $2,190,294 — but each distinct violation type carries its own cap. A practice with unencrypted voicemail storage, no BAA, and no audit logging isn't facing one violation category. It's facing several.
These penalties don't require a breach to trigger. An unencrypted voicemail inbox or a missing BAA is enough — the gap itself is the violation.
HIPAA Compliance Requirements for VoIP Systems
The HIPAA Security Rule organizes its requirements into three safeguard categories. Each applies directly to a VoIP deployment.
Administrative Safeguards
These require documented policies governing how staff handle PHI on communication systems, designated security responsibility, and workforce training. Training isn't optional — it's a specific requirement, and using a new VoIP system without training staff on PHI handling creates an administrative safeguard gap.
Physical Safeguards
These govern physical access to devices that store or transmit PHI — desk phones, headsets, computers running softphone apps, and the servers or cloud infrastructure hosting the VoIP platform.
Technical Safeguards
This is where most of the VoIP-specific requirements live. Under 45 CFR 164.312, covered entities must implement:
- Access controls — unique user IDs, emergency access procedures, automatic logoff
- Audit controls — mechanisms to record and examine activity in systems containing ePHI
- Integrity controls — protections against unauthorized alteration of ePHI
- Person or entity authentication — verifying that users are who they claim to be
- Transmission security — protecting ePHI transmitted over electronic networks
Encryption under the Security Rule is classified as "addressable" — meaning you must assess whether it's reasonable and appropriate, implement it if so, or document why you chose an equivalent alternative. For any modern VoIP deployment, not encrypting calls and stored voicemails is indefensible.
Audit Trail Requirements
HIPAA requires covered entities to identify who accessed what information, when, and from where. For VoIP, this means the system must generate logs covering authentication events, call detail records, voicemail access, configuration changes, and data exports. These logs must be retained and available for compliance audits.
Compliance as Shared Responsibility
Those audit logs also clarify something broader: HIPAA compliance is never one party's problem. The healthcare organization owns policies, user access management, training, and risk management. The VoIP vendor is responsible for providing a secure platform and signing a BAA. Both sides are accountable — and neither can substitute for the other.
E911 Requirements
Multi-site practices and organizations with remote or hybrid staff must address E911 compliance under Kari's Law and RAY BAUM's Act. Key requirements include:
- Direct 911 dialing — no access prefix required, for systems manufactured or installed after February 16, 2020
- Dispatchable location for fixed VoIP — street address plus floor, suite, or room number, as of January 6, 2021
- Nomadic/non-fixed users — automated dispatchable location required where technically feasible (softphone users working from home or offsite locations)
Static E911 configurations fail for remote workers not physically at the registered address — a critical gap for any hybrid healthcare team.
Security Features Every Healthcare VoIP System Must Have
Encryption Standards
- In transit: TLS 1.2 or 1.3 for SIP signaling, SRTP for call media
- At rest: AES encryption for stored voicemails, recordings, and transcripts (AES-128, AES-192, and AES-256 are all FIPS 197-recognized — AES-256 is not the only compliant option, but any of these must be applied consistently)
- Red flag: Any provider that lists encryption as an optional add-on rather than a default should be removed from consideration
Access Controls and Authentication
- Role-based access control (RBAC) limits which staff can access recordings, voicemails, configuration settings, and analytics
- Multi-factor authentication (MFA) should be required for all administrative portals and mobile apps
- Least-privilege principles should govern every user role — staff should only see what their function requires
Audit Logging
A sufficient audit trail is timestamped, tamper-resistant, and covers:
- Authentication events (logins, failed attempts)
- Call detail records
- Voicemail access and retrieval
- Configuration changes
- Data exports
Logs must be retained and accessible for compliance reviews.
Secure Call Recording Governance
Blanket call recording is not automatically safe. Recordings containing PHI must be:
- Encrypted at rest
- Access-restricted by role
- Subject to defined, enforced retention periods
- Available for legal hold when required
On-demand or queue-specific recording is preferable to recording every call indiscriminately.
Network-Level Protections
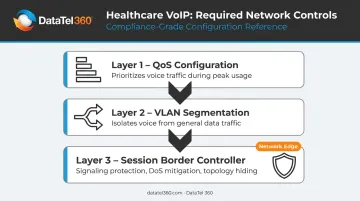
The VoIP platform is only as secure as the network beneath it. A compliant deployment requires three infrastructure controls:
- Prioritize voice traffic with QoS configuration to prevent call degradation during peak usage
- Isolate voice from general data traffic using VLAN segmentation
- Deploy Session Border Controllers (SBCs) at the network edge for signaling protection, denial-of-service mitigation, and topology hiding
Bandwidth planning deserves its own attention. Cisco's documentation shows meaningful differences between codec choices:
| Codec | Bandwidth Per Concurrent Call | Notes |
|---|---|---|
| G.711 | 87.2 kbps | Ethernet, 20 ms payload; includes IP/UDP/RTP/L2 headers |
| G.729 | 31.2 kbps | Same assumptions; ~64% lower bandwidth |
The commonly cited 85–100 kbps planning range applies to G.711. Know your codec and your concurrent call count before sizing your connection.
Healthcare Workflow Capabilities That Support Patient Care
Security controls matter — but a healthcare VoIP system also has to work for the people using it.
Intelligent Call Routing
Advanced routing by department, specialty, urgency, language, or time of day reduces hold times and gets patients to the right person faster. Legacy systems that funnel every call to a single front-desk line create exactly the bottlenecks patients complain about. Among practice managers surveyed by MGMA for 2026 priorities, 22% named phone access and 21% named wait times as their top patient-access concerns. Intelligent routing directly solves both.
EHR and Practice Management Integration
Properly configured EHR integration delivers real workflow benefits:
- Screen pops that surface patient records when a call arrives
- Click-to-call from within a patient chart
- Automatic call logging to the patient encounter record
Misconfigured integrations, however, can create unauthorized PHI pathways. Scope and configure carefully — and confirm compatibility with your specific EHR platform (Epic, Cerner, athenahealth, or others) directly with the vendor before signing a contract.
Mobile Access and After-Hours Coverage
Softphone apps let physicians and on-call staff place and receive calls from personal devices while displaying the practice's main number as caller ID. For this to be compliant, three conditions must be met:
- Mobile app usage is explicitly covered in the BAA
- Calls are subject to the same encryption controls as desk phones
- Access is governed by the same identity and authentication policies
That setup keeps personal cell numbers private, staff reachable, and the practice covered.
How to Evaluate and Implement Secure VoIP in Your Practice
Build Your Evaluation Framework First
Before contacting vendors, document:
- Current communication workflows and where PHI is touched
- Which EHR or practice management systems must integrate
- Uptime and reliability requirements
- Number of users and locations
- Whether telehealth or multi-site routing is needed
This prevents vendors from overselling features that don't match your workflows.
Demand Verifiable Evidence
Marketing claims aren't enough. Require any shortlisted provider to:
- Produce a signed BAA covering all planned features — including voicemail, recording, and analytics
- Share encryption standards in writing
- Provide SOC 2 or equivalent audit documentation
- Describe their breach notification timeline and process
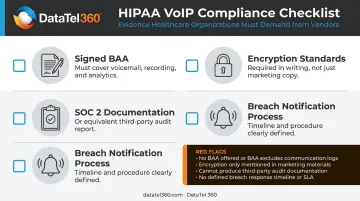
Walk away from any provider with no BAA, a BAA that excludes core features, vague encryption language, or no audit trail capabilities.
Plan Network Readiness and Phased Deployment
- Assess bandwidth, jitter, and latency before go-live
- Configure QoS to prioritize voice traffic
- Run a pilot with one department or location to test call flows, after-hours routing, and failover
- Verify E911 location data for every office address and remote worker configuration
DataTel 360 works with healthcare organizations across the Southeast on this kind of deployment planning, from pre-installation network assessment through phased rollout and 24/7 ongoing support.
Train Staff Before and After Go-Live
Staff must understand:
- Which channels are approved for patient communication
- How to use secure voicemail and mobile apps correctly
- What constitutes a potential breach and how to report it
This is a HIPAA administrative safeguard requirement. Training is built into compliance, not bolted on afterward.
Frequently Asked Questions
What makes a VoIP system HIPAA-compliant?
HIPAA compliance requires three components: technical controls (encryption in transit and at rest, role-based access, audit logging), a signed Business Associate Agreement with your provider, and internal policies governing staff use. All three are required. None is sufficient on its own.
Do healthcare providers need a Business Associate Agreement with their VoIP provider?
Yes — a BAA is legally required whenever a vendor handles, transmits, or stores PHI on your behalf. Using a VoIP system for patient communications without a signed BAA constitutes a HIPAA violation, regardless of any technical security measures in place.
Can VoIP systems integrate with EHR and practice management software?
Many healthcare VoIP platforms support EHR integrations for screen pops, click-to-call, and automatic call logging. Integration must be carefully configured to limit PHI exposure. Confirm compatibility with your specific EHR with any vendor before selecting a platform.
What are the risks of using a standard or consumer VoIP system in a healthcare setting?
Standard VoIP systems typically lack encryption standards, audit logging, and BAA availability. Using them to handle patient calls or voicemails exposes the practice to HIPAA civil monetary penalties and data breach liability — even if no breach actually occurs.
How much internet bandwidth does a healthcare VoIP system require?
Plan for approximately 87.2 kbps per concurrent G.711 call, based on Cisco's calculations including all protocol overhead. G.729 requires less at 31.2 kbps. Dedicated bandwidth with QoS configuration is necessary to prevent call quality degradation during peak usage.
Is VoIP reliable enough for emergency and critical healthcare communications?
Enterprise-grade healthcare VoIP systems include geo-redundant infrastructure, failover routing, and high-availability SLAs. Reliability depends on both the provider's uptime guarantees and the practice's own internet redundancy. A secondary failover circuit is strongly recommended for any clinical environment.


